WHO Pushes Experimental Ebola Treatments and Vaccines Into Trials as Bundibugyo Outbreak Spreads — Racing Against a Deadly Clock
In the shadow of one of the world’s most feared viruses, the World Health Organization is moving fast. On Thursday, the agency identified three promising experimental treatments to prioritize against the Bundibugyo strain of Ebola currently flaring up in the Democratic Republic of Congo and spilling into Uganda. The message is clear: no approved drugs or vaccines exist specifically for this strain, so the only responsible path forward is rigorous clinical trials — and fast.
The three treatments getting top billing are:
- Mapp Biopharmaceutical’s MBP134
- Regeneron’s maftivimab
- Gilead Sciences’ antiviral remdesivir (the same drug that gained fame during COVID)
Regeneron already has supplies of maftivimab on the ground in the DRC, ready to go if needed for immediate compassionate use or trial integration. For prevention, Gilead’s experimental oral antiviral obeldesivir is being eyed for post-exposure protection for close contacts — assuming strong contact tracing can actually happen in the affected regions.
{kind=link}
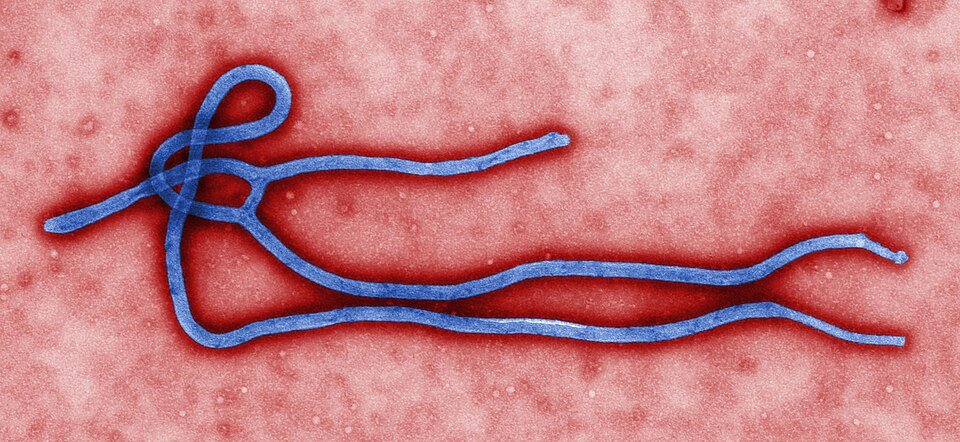
This colorized transmission electron micrograph (TEM) revealed some of the ultrastructural morphology displayed by an Ebola virus virion. See PHIL 1832 for a black and white version of this image.
Where is Ebola virus found in nature?The exact origin, locations, and natural habitat (known as the “natural reservoir”) of Ebola virus remain unknown. However, on the basis of available evidence and the nature of similar viruses, researchers believe that the virus is zoonotic (animal-borne) and is normally maintained in an animal host that is native to the African continent. A similar host is probably associated with Ebola-Reston which was isolated from infected cynomolgous monkeys that were imported to the United States and Italy from the Philippines. The virus is not known to be native to other continents, such as North America.
On the vaccine side, a single-dose candidate called rVSV Bundibugyo (developed by the International AIDS Vaccine Initiative) looks most promising, but it won’t be ready for trials for another seven to nine months. A faster option from Oxford University and the Serum Institute of India could potentially enter testing in two to three months. Meanwhile, Merck’s existing Ervebo vaccine — the only licensed Ebola shot — won’t be used outside trials because evidence it works against Bundibugyo remains shaky.
This isn’t panic mode — yet. But with hundreds of suspected cases and deaths already reported, the WHO and partners like Africa CDC are working with Congolese and Ugandan authorities to design ethical, high-quality trials under pressure. Combination therapies (monoclonal antibodies plus remdesivir) are also on the table.
Ebola has a nasty habit of reminding us how fragile global health security really is. Different strains behave differently, and while we’ve made huge progress since the devastating 2014–2016 West Africa outbreak, each new flare-up exposes gaps — especially for less common variants like Bundibugyo. The fact that we’re still relying on experimental tools in 2026 shows both how far we’ve come (we actually have candidates ready to test) and how far we still have to go.
What stands out here is the WHO’s insistence on trials rather than rushing unproven treatments into widespread use. In past outbreaks, the urgency sometimes blurred ethical lines. This time, they’re trying to do it right: gather real data while saving lives. That balance is tough when people are dying, but it’s the only way to build tools that actually work long-term.
For the communities on the front lines, this outbreak brings fear, border closures, and the usual heartbreak. For the rest of the world, it’s another reminder that deadly pathogens don’t respect borders — and that investment in preparedness (and equitable access to these future tools) matters.
Here’s hoping the trials deliver clear answers quickly, and that this outbreak is contained before it spirals further. Global health wins are rarely flashy, but they’re some of the most important ones we can get.
What do you think — does hearing about these rapid-response efforts make you more confident in our ability to handle outbreaks, or does it highlight how reactive we still are? Either way, fingers crossed for good data and better outcomes ahead.